The Insightful Orthotics App
*The Insightful Orthotics app is currently compatible with iPhones only, not Android. iPad users will also be able to access it providing they have a structure scanner on their iPad. The app’s scanning function utilizes the front facing camera as its accuracy is much better than the rear facing camera.
Quantification of Arch
Height In a Foot Orthotic: Defining a Standardized Methodology
The longitudinal arch height of foot orthotic is one of the more important elements, yet a standard of measurement has not been defined. This author proposes a standard way to quantify orthotic arch height, defining a quantification technique for foot orthotics called Longitudinal Arch Height and its Distal Position.
This article was first published in the Lower Extremity Review in September of 2020.
By Ian Engelman
The absence of common measurement practices for and subsequent fabrication of foot orthotics has produced a wide variety of orthotic contour outcomes, resulting in inconsistent ideas about how to obtain good clinical results. For those who are experts in the profession, it is fair to suggest that the longitudinal arch height of a foot orthotic is one of the more important elements, yet a standard of measurement has not been defined. Indeed, determining the amount of support needed in this area is hard to discuss without an index or a way to measure it. In the following, we at Insightful Products, LLC., propose a standard way to quantify orthotic arch height, defining a quantification technique for foot orthotics called Longitudinal Arch Height and its Distal Position. Quantification of anatomical arch height is a different discussion, though it is briefly reviewed.
Science and quantification are long overdue in the orthotic work that we do on a daily basis. The process of capturing the anatomical arch, creating a positive model, and managing arch fill has been solely a decision of those trained in the art. There cannot be an index of exactly how much correction we are using in a custom foot orthotic without quantification.
A technique for defining the longitudinal arch height (LAH) parameter should take special consideration of which part of the body of the orthotic is most effective for the management and restoration of the architecture of the foot. To determine the most effective area for support of the medial column of the foot, it is helpful to think about the weight line through the tibia.
The Role of the Talus
It is well understood that the fibula is not a weight-bearing bone, which leaves the tibia to support the entire weight of the body above the knee. The talus is the only bone that directly supports the tibia. Under most circumstances, the talus is not a contact point with the ground or the inside sole of the shoe. Rather, movement force is distributed through the talus to the navicular and calcaneus. A plethora of tarsal ligaments keeps the talus from crushing downward through the middle of the foot while supporting the body’s weight. Over time, without a foot orthotic, ligaments stretch with weight or become lax with age and the anatomical longitudinal arch drops lower. A term commonly used to describe the change is Adult Acquired Flatfoot Deformity
(AAFD).
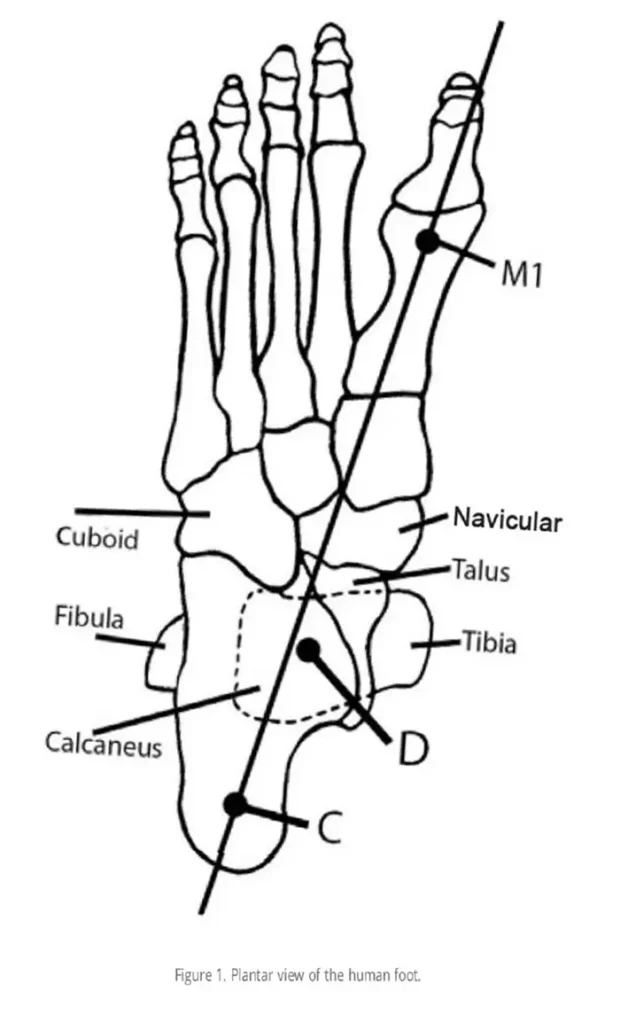
Some of the force is transferred to the navicular, but the talus is primarily supported by the calcaneus. Because the talus is anterior to the contact point of the calcaneus, there is a plantarflexion moment of force on the calcaneus in stance phase. A series of ligaments is primarily responsible for maintaining the calcaneal pitch. From the plantar view, the four major tarsal bones seem to intersect: cuboid, calcaneus, navicular and talus (Figure 1). The series of ligaments that connect the tarsals create a “hammock” type of support for the forces that run through the center of the tibia onto the talar dome. In Figure 1, point D represents the center of the tibia transposed onto the talar dome.
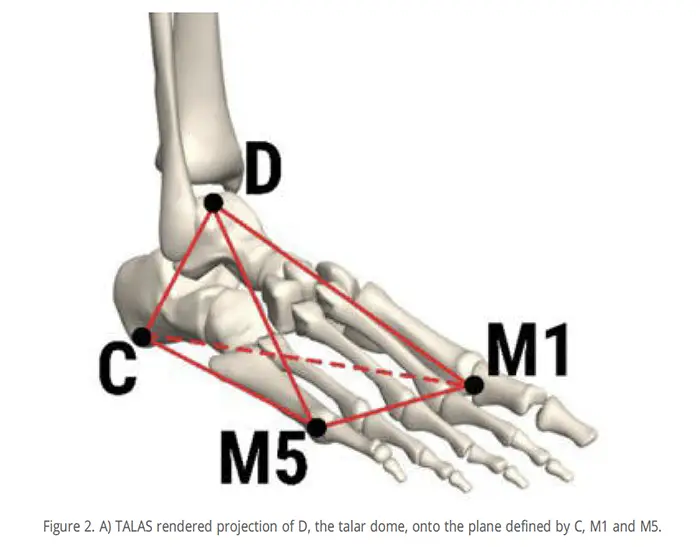
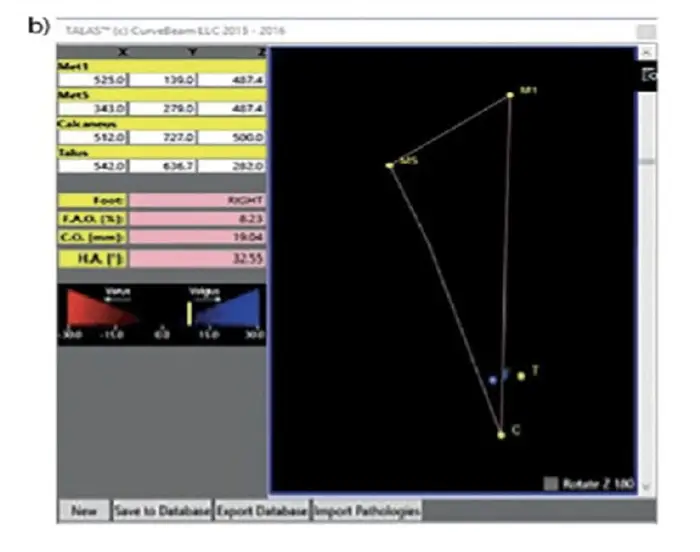
The talar dome is a standard point of reference for 3 dimensional (3D) AAFD analysis called Foot Ankle Offset (FAO).¹ The recent advent of weight-bearing computed tomography (CT) scans and 3D rendering has enabled the advent of TALAS™ software plugin for CubeView™ (Torque Ankle Lever Arm System; CurveBeam, Hatfield, PA). This CurveBeam 3D-rendering technology affords a repeatable measure (Figure 2, 3)2 of the stability of the foot that projects the center of the talar dome (D) onto the base of support that can be defined by three points: first metatarsal head (M1), fifth metatarsal head (M5) and the calcaneus (C). Studies have shown that this measurement technique is reproducible, and that Talas is a reliable clinical index. 3D-CT scans and semi- automated analysis3 allow positioning of reproducible 3D anatomical landmarks. Through this work, methods have been refined so that there is a high accuracy of determining M1, defined with cut slabs as the lowest point of the metatarsal head. A similar definition for the location of the calcaneus, C, is defined by the lowest point of the calcaneus. Talas uses the top of the talar dome at its coronal plane midpoint, D. This point sits squarely under the distal end of the tibia, which is where the ground reaction forces direct in single limb stance. Studies show that these landmarks represent the most reproducible location for the Foot Ankle Offset (FAO) index. The FAO index seems to be the best metric yet for evaluation of the severity of AAFD.
However, our focus is on a quantification technique for foot orthotics, not for feet. Efforts to quantify anatomical arch height have been made for decades. Each has its unique set of challenges.4 Another reproducible method for measuring both flat feet and AAFD is a navicular height at full single limb stance. Other methods do exist, but, in our opinion, most are dubious at best. The techniques of measuring the anatomical contours for a patient for the orthotic impression also vary, and so do the results. More research needs to be done to determine which methods are best for accurate foot arch impressions. For the orthotic, however, the LAH index for orthotic arch height does provide a reliable measure from which clinical outcomes can start to be evaluated. As we look at the projection of the talar dome onto the line C-M1 (Figure 2), there are two things to think about for orthotic management of the foot:
- the proximity to C-M1 line in the medial/lateral direction, and
- the distal position (DP) of the point D in the anterior/posterior direction
How Much Support
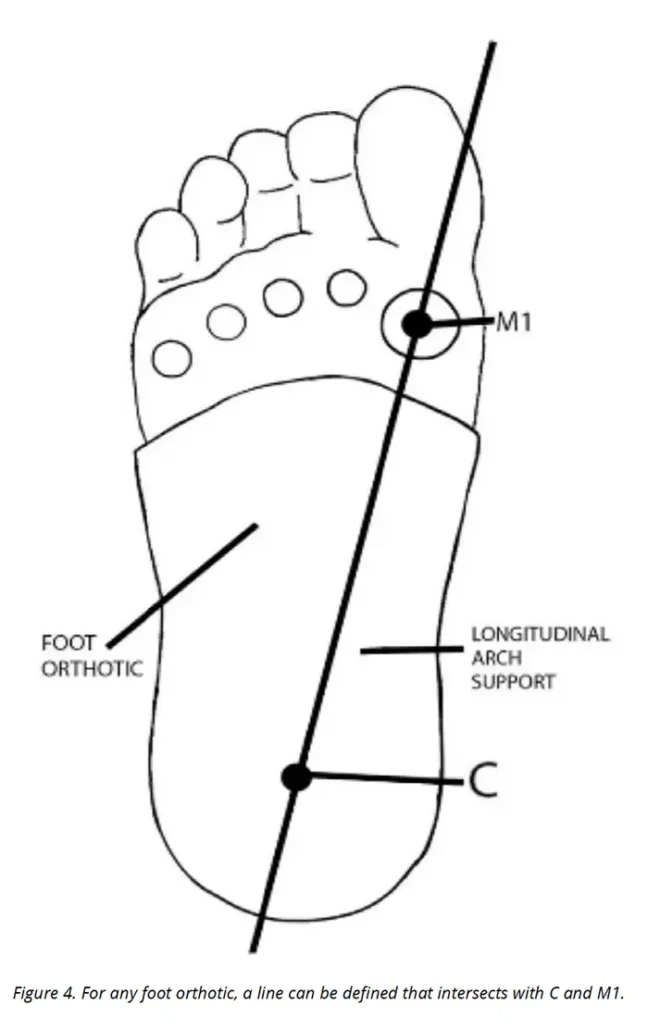
It would seem ideal to support the foot directly below the distal tibia, or approximately in the middle of the talar dome, D. For orthotic treatment it is clinically advantageous to know how much support is being provided to the patient. A technique for providing that parameter is described here. For the foot orthotic, C is defined as the deepest part of the “well” or heel cup, which is traditionally bisecting the heel pad in the sagittal and coronal planes (Figure 4). From the plantar view, one can draw a straight line from the calcaneus to the first metatarsal head. This reproducible line is approximately crossed by the vector of the ground reaction forces described and validated by the studies using the Talas method. The calcaneus and first metatarsal points, M1 and C, are reasonably transferred to the orthotic for those skilled in the art (see Figure 2). For those familiar with the field of foot orthotics, the likely position of the first metatarsal head relative to the foot orthotic is accurate enough to produce meaningful metrics. Small differences of determining these points (M1 and C) between practitioners might result in slight angular variance. This might lead to a LAH error of +/- a few millimeters. For standard orthotic evaluation, we believe that these measurement variations are within a small enough tolerance to ensure clinical value.
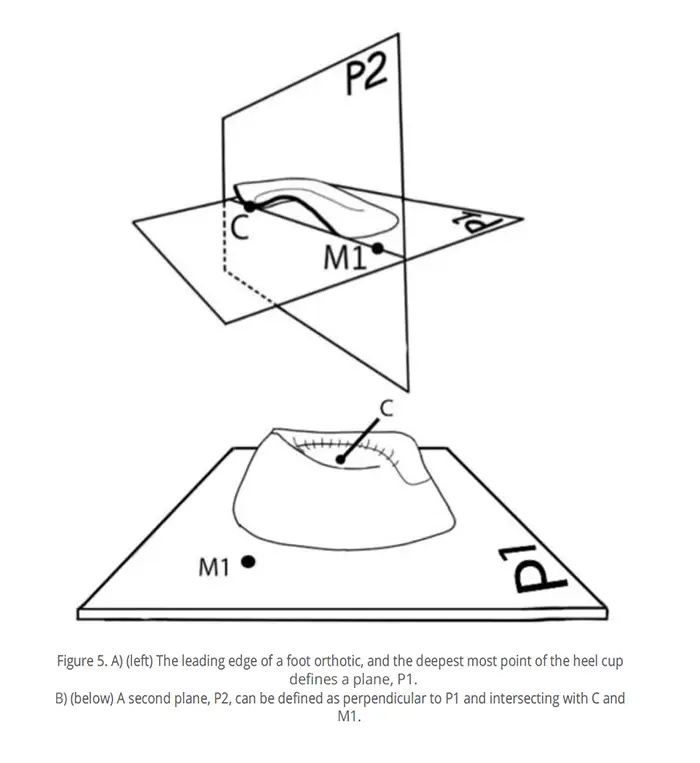
The leading edge of a foot orthotic along with the heel cup defines the location of a support plane. If you put an orthotic on a table, most designs will rest with the front edge lined up with the table. This table-top surface is defined here as Plane 1 (P1; Figure 5B).
A second plane, P2, can be defined as perpendicular to P1 and intersecting with the line M1-C, Figure 5A. This plane passes through the orthotic near or at the most mechanically effective location for corrective pressure, in the specific area atop the talar dome, D.
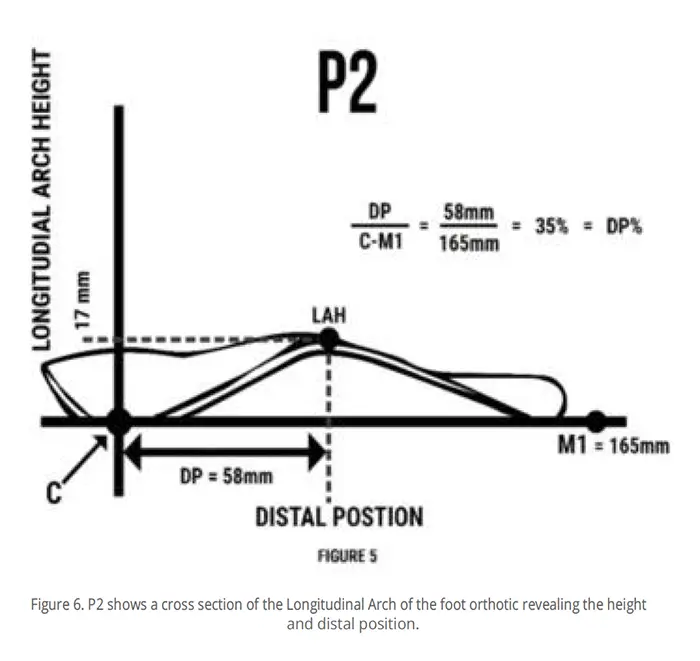
The P2 plane will reveal a curve that traces the curvature of the longitudinal arch (LA) and will have a maximum height above P1. Figure 6 shows that maximal position, termed Longitudinal Arch Height (LAH). In this example, that value is 17mm. The DP of LAH along the M1-C line is also clinically relevant. Figure 6 shows a DP of 58mm. In order to find a guide that will work for many patients, we need a parameter that will take individual variation of foot length into account. In that effort, the DP of the longitudinal arch is best described as a percentage of foot length. The distance from C to M1 is the natural and reliable choice of reference. Here DP = 58mm, with a C– M1 length of 165mm; 58mm/165mm gives us a DP percentage of 35%.
Since quantification of foot orthotics is just now being defined and considered, logically, there cannot possibly exist supporting studies for best LAH location. However, we can begin by thinking about the location of the ground reaction forces. It is reasonable to suggest that a LAH that is closest to the talar force vector, D, is the best corrective location. With this new index, we can start to determine the best DP% for correction that is also most tolerable to the wearer. Our professional judgement and clinical outcome experience show that an excellent location for distal position is 35%.
Predictable Outcomes
One might argue that the height of just one point on the foot orthotic does not fully represent the supportive curvatures. For instance, it is possible to construct an orthotic with a spike to make a localized maximum height. Clearly this type of arrangement would not be tolerable to the wearer, and a broader support will be required for compliance. Additionally, for most orthotic contours, there are likely to exist other contact points that are more medial and with greater distance from the P1 plane. If measured, these values would be greater in height. Although this is true, it is also true that any points more medial will be further away from the center of gravity force vector, D, and therefore less clinically meaningful.
Beyond a quantification tool for the orthotic arch height, a reliable methodology for quantification of the anatomical arch height is equally relevant for predictable outcomes. The current variation in techniques for taking an impression or scanning compromises the reproducibility of anatomical arch measurements for the orthotic manufacturer. We have developed what initially seems to be an accurate non-weight bearing scanning technique for consistent clinical outcomes. From reliable anatomical data, we can start to provide a truly scientific quantifiable relationship between the anatomical arch height and the orthotic arch height. This can be described as a percentage. As an application tool, it allows clinicians to more specifically prescribe the degree of the most important element of foot orthotic care, the Longitudinal Arch.
With time and experience, the profession will now be able to use a LAH metric and DP% that will allow case to case outcome comparisons; furthermore, this metric can provide a basis for gauging effective, comfortable, and meaningful corrective contours for foot orthotic treatment.
Ian Engleman has been president of Insightful Products, LLC, for more than 17 years. The Maine-based company specializes in the design and fabrication of orthopedic braces to help people walk.
References
1. Lintz F, Welck M, Bernasconi A, et al. 3D biometrics for hindfoot alignment using weightbearing CT. Foot Ankle Int. 2017;38(6):684-689.
2. Lintz F, Netto CC, Barg A, Burssens A, Richter M, Weight Bearing CT International Study Group. Weight-bearing cone beam CT scans in the foot and ankle. EFORT Open Rev. 2018;3(5):278-286.
3. De Cesar Netto C, Bang K, Mansur NS, et al. Multiplanar semiautomatic assessment of foot and ankle offset in Adult Acquired Flatfoot Deformity. Foot Ankle Int. 2020;41(7):839-848.
4. Williams DS, McClay IS. Measurements used to characterize the foot and the medial longitudinal arch: reliability and validity. Phy Ther. 2000;89(9):864-71.